

Introduction
A majority of patients with diffuse large B cell lymphoma (DLBCL) will be cured with frontline chemoimmunotherapy, however a significant number of patients will relapse. Although autologous haematopoietic stem cell transplantation (autoHCT) may lead to sustained survival in some relapsing patients, long term survival with relapsed DLBCL is approximately 25% (Larouche et al., J Clin Oncol 2010;28(12):2094).
Allogeneic HCT (alloHCT) is a potential treatment strategy in some DLBCL patients with relapsed disease. We performed a retrospective national registry study to examine alloHCT practice and outcomes for DLBCL in Australia and New Zealand in the modern era.
Methods
Data was collected through the Australasian Bone Marrow Transplant Recipient Registry (ABMTRR) for patients receiving an alloHCT for DLBCL between January 2009 and December 2019. Survival was analysed using the Kaplan-Meier method, with comparisons between the transplant periods 2009-2014 and 2015-2019 performed using the log-rank test. Both univariate and Cox proportional hazards regression were performed to determine significant risk factors for transplant outcome. The following risk factors were analysed for impact on outcomes: age, transplant before 2015, previous autoHCT, remission status at transplant, use of myeloablative conditioning (MAC), haploidentical donor (HD) and use of T cell depletion (TCD).
Results
A total of 154 patients were included in the analysis. The median age was 52 years (range 19-71) and 68% were male. Disease status at transplant was complete remission (CR) in 49%, partial response in 31% and stable or progressive disease in 17% (missing data in 3%). Fifty-five per cent had undergone a previous autoHCT. Approximately equal proportions of donors were HLA-matched siblings or matched unrelated (45% and 46% respectively) and 9% were HDs. MAC was utilised in 26%, and TCD in 24% (alemtuzumab in 3%, anti-thymocyte globulin in 21%) (data missing in 12%). The median times to neutrophil engraftment and platelet engraftment were 16 and 18 days respectively.
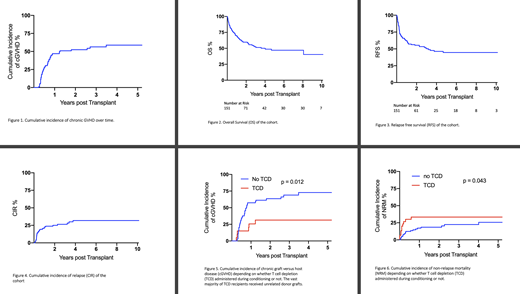
Non-relapse mortality (NRM) at 1-year and 5-years was 20% (95%CI 7-30%) and 26% (95%CI: 13-38%). The 100-day cumulative incidence of grade II to IV acute graft versus host disease was 15% (95%CI 5-31%). The 3-year cumulative incidence of chronic graft versus host disease (cGVHD) was 56% (95%CI 46-65%) (figure 1).
The median duration of follow up for the cohort was 3.98 years (range 0-9.64 years). Median overall survival (OS) post-transplant was 4.01 years, with 5-year OS of 47% (95%CI 38-56%) and 10-year OS of 40% (95%CI 26-54%) (figure 2). The 5-year relapse free survival (RFS) was 45% (95%CI 26-50%) (figure 3). The cumulative incidence of relapse (CIR) was 21% at 1 year and 32% at four years, however relapses were not seen after this point, suggesting a subpopulation with durable remissions (figure 4).
On univariate analysis, TCD was associated with both reduced incidence of cGVHD (HR 0.35 95%CI 0.19-0.66, p=0.012) and increased NRM (HR 2.10 95%CI 0.88-4.99 p=0.043). These associations were maintained on multivariate analysis (MVA) (HR 0.29 95%CI 0.16-0.76, p=0.011; HR 2.19 95%CI 1.02-4.70, p=0.045) (figures 5, 6). TCD did not impact on RFS. The vast majority of TCD was given in unrelated donor alloHCTs. CR at time of transplant was associated with improved RFS on univariate analysis (HR 1.65 95%CI 1.04-2.64, p=0.034), however this association was not seen on MVA. No other analysed risk factors impacted OS, RFS, NRM, CIR or GVHD rates on either univariate or MVA.
An average of 14 alloHCTs were performed each year, with a trend towards increasing annual numbers over time. There was a significant increase in the proportion of haploidentical transplants between 2009 and 2019 (p=0.003), though total numbers were low (n=14). There was no significant change over time for the use of MAC, TCD, nor in OS, RFS or NRM.
Conclusion
There has been an increase in the rates of alloHCT with HDs for DLBCL in Australia and New Zealand over the past decade. Survival and relapse rates are relatively favourable compared to the published literature, with sustained remissions observed (5 and 10-year OS of 47% and 40% respectively). TCD is associated with reduced cGVHD rates, as well as increased NRM. Ongoing reporting of alloHCT outcomes in DLBCL is important given the emerging role of novel therapies such as bispecific monoclonal antibodies and chimeric antigen receptor T cell therapy.
Di Ciaccio:Jansen: Honoraria, Other: travel and accomodation grant. Greenwood:Servier: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; MSD: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Spencer:Celgene, Janssen and Takeda: Speakers Bureau; AbbVie, Amgen, Celgene, Haemalogix, Janssen, Sanofi, SecuraBio, Specialised Therapeutics Australia, Servier and Takeda: Honoraria; Amgen, Celgene, Haemalogix, Janssen, Servier and Takeda: Research Funding; AbbVie, Celgene, Haemalogix, Janssen, Sanofi, SecuraBio, Specialised Therapeutics Australia, Servier and Takeda: Consultancy. Arthur:Royal North Shore Hospital: Current Employment. Hamad:Novartis: Honoraria; Abbvie: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal